Knowledge of ASHA workers about maternal and child health services in Mysuru
Sugandha B.K.1, Jagannath P.2*
DOI: https://doi.org/10.17511/ijphr.2019.i4.06
1 B K Sugandha, K S Hegde Medical Academy Nitte Deemed to be University, Mangalore, Karnataka, India.
2* Jagannath P, Head of the Department, Department of Public Health, K S Hegde Medical Academy Nitte Deemed to be University, Mangalore, Karnataka, India.
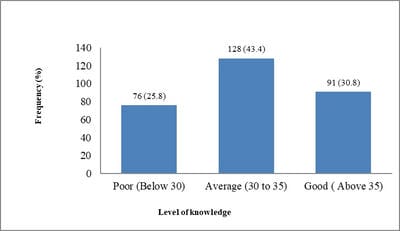
Background: Accredited Social Health Activist (ASHA) programme has been accepted, and the services utilization has been increased among many Indian communities since its inception in 2005 under National Rural Health Mission (NRHM). ASHA worker's knowledge is important for the success of this program. Objectives: To assess the level of knowledge of ASHA workers about Maternal and Child Health (MCH) services. To determine the association between socio-demographic characteristics and the level of knowledge of ASHA workers about Maternal and Child Health services. Methods and Material: A cross sectional study was conducted among 295 ASHA workers of Mysuru Taluk, Karnataka from January to April 2019. Sample size was calculated based on the estimation of proportions method and all the ASHA workers were selected randomly. The semi-structured self-administered questionnaire formulated based on the ASHA modules and translated into the local language (Kannada) was used for data collection. Descriptive data was analyzed by using frequency, percentage, mean and standard deviation. For the association between variables, Chi-square / Fisher’s exact test was used. Results: Knowledge about Antenatal Care was average among half (51.5%) of the participants. All the listed danger signs during pregnancy were identified only by 49.5% of ASHA workers. About 50% of the respondents were not aware of the exclusive breastfeeding till six months after birth. Conclusions: Knowledge levels about maternal and child health services were found to be average in most of ASHA workers.
Keywords: Accredited Social health Activist, Community Health Workers, Maternal and Child Health, National Health Mission, Knowledge
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Head of the Department, Department of Public Health, K S Hegde Medical Academy Nitte Deemed to be University, Mangalore, Karnataka, India. Email:  |
Sugandha BK, Jagannath P. Knowledge of ASHA workers about maternal and child health services in Mysuru. Public Health Rev Int J Public Health Res. 2019;6(4):169-176. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/116 |
 |
 ©
©