Role of Nurses in Maternal and newborn Care at Community Health Centers of Rural and Tribal areas of Madhya Pradesh, India
Verma M1*, Maitra S2, Gedam S3
DOI:https://doi.org/10.17511/ijphr.2024.i01.01
1* Mamta Verma, PhD, Associate Professor, Nursing College All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
2 Shubhada Maitra, PhD Professor, School of Social Work, Tata Institute of Social Sciences, Mumbai, Maharashtra, India.
3 Sharad Gedam, Associate Professor, Department of Pediatrics, ABV Government Medical College, Vidisha, Madhya Pradesh, India.
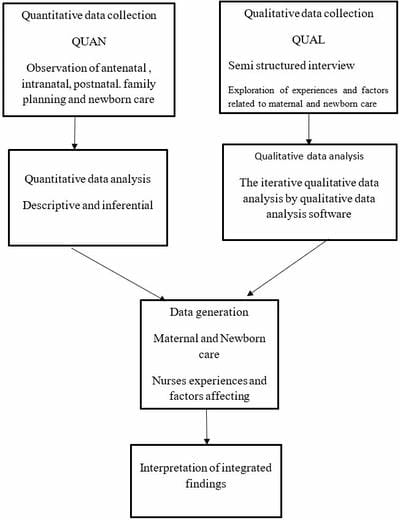
Introduction: The study is an attempt to observe maternal and newborn care provided by nurses at CHCs, understand their experiences and what barriers and facilitators they encountered. Material and methods: The study was carried out at two rural and two tribal CHCs. A convergent mixed-method research approach was used. The observational method was adopted to observe maternal and newborn care. The phenomenology method was followed to understand experience, barriers and facilitators. Descriptive data analysis reveals that nurses are providing comprehensive antenatal, intranatal and newborn care however certain important post-natal nursing care were missing. Iterative Qualitative analysis through ATLAS.ti has captured themes of experiences about challenging night shifts, safety threats, inter and intra-professional hierarchal issues, multitasking, professional issues and social isolation. Results: Results of the study identified barriers related to human resources, inadequate basic facilities, and nurses-related, culturally related, interprofessional issues. Facilitators consist of nurses’ skills and competencies, good facilities and a labour room. Maternal and newborn care was performed by nurses however few gaps were identified. Conclusion: Nurses have a variety of interconnected experiences in rendering maternal and newborn care at CHCs. Nurses encounter several barriers and facilitators in maternal care.
Keywords: Maternal Care, Newborn Care, Rural, Tribal, Community Health Centers, Nurses, Role
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , PhD, Associate Professor, Nursing College All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India. Email:  |
Verma M, Maitra S, Gedam S. Role of Nurses in Maternal and newborn Care at Community Health Centers of Rural and Tribal areas of Madhya Pradesh, India. Public Health Rev Int J Public Health Res. 2024;11(1):1-11. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/187 |
 |
 ©
©