Food habits and Nutritional status among school-going Adolescents of Dhaka City, Bangladesh
Ahmed FA1*, Sadia SA2, Mkpa BO3, Afroz S4, Islam MT5
DOI:https://doi.org/10.17511/ijphr.2024.i02.01
1* Ferdous Ara Ahmed, Student, Public Health, Monroe University Usa and Bachelor of Medicine and Surgery University of Dhaka, Bangladesh.
2 Shima Ali Sadia, student, Public Health, Monroe University USA and Bachelor of medicine and surgery University of Dhaka, Bangladesh.
3 Beatrice Onyinyechi Mkpa, Student, Public Health, University of Nigeria Nsukka and Monro University, Bangladesh.
4 Sadia Afroz, Student, Public Health, Dhaka University and Monroe University, Bangladesh.
5 Mussa Tasmiah Islam, Student, Public Health, Govt College Sylhet Bangladesh and Monroe University, Bangladesh.
Background: Adolescent nutrition represents a critical public health concern in rapidly urbanizing areas of Bangladesh, yet comprehensive data on the nutritional status and food habits of urban school-going adolescents remain limited. This study aimed to assess the nutritional status and food habits among school-going adolescents in Dhaka City, Bangladesh.
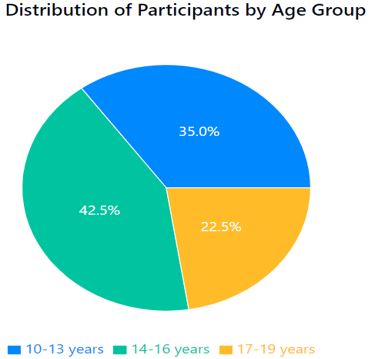
Methods: A cross-sectional study was conducted among 120 school-going adolescents (aged 10-19 years; 52.5% females) from four schools in Dhaka City. Anthropometric measurements were taken following WHO standardized procedures. Food habits were assessed using a food frequency questionnaire and 24-hour dietary recall. Nutritional status was classified using WHO AnthroPlus software based on BMI-for-age Z-scores. Socioeconomic data and physical activity levels were collected using structured questionnaires.
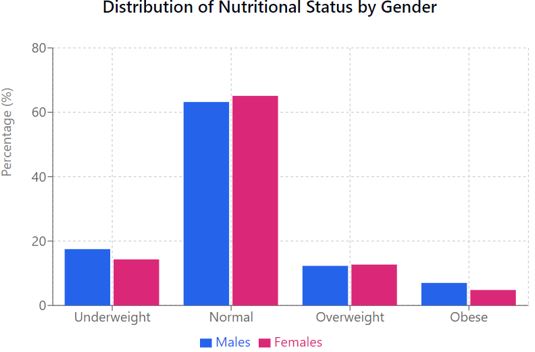
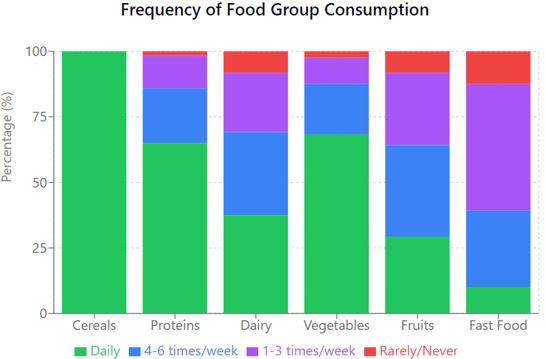
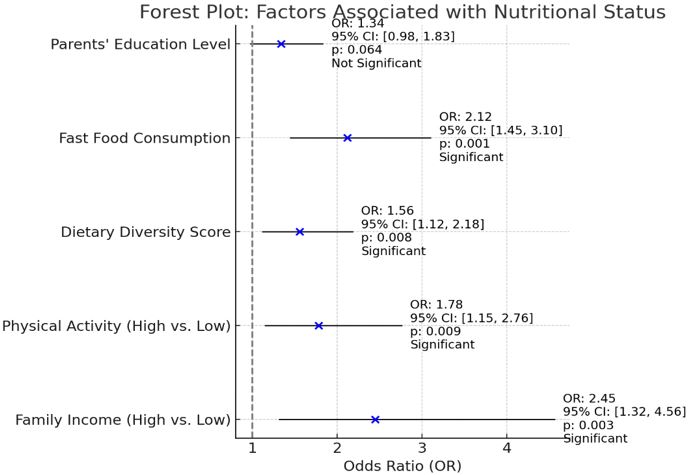
Results: The study revealed a dual burden of malnutrition, with 15.8% of adolescents being underweight and 18.3% overweight or obese. Meal skipping was prevalent (35%), with breakfast being the most commonly skipped meal (23.3%). The mean dietary diversity score was 5.8 ± 1.4 out of 9 food groups. Significant associations were found between nutritional status and family income (OR: 2.45, 95% CI: 1.32-4.56, p=0.003), physical activity levels (OR: 1.78, 95% CI: 1.15-2.76, p=0.009), and fast food consumption (OR: 2.12, 95% CI: 1.45-3.10, p=0.001). Gender disparities were observed in physical activity patterns and dietary choices, with females showing lower participation in high-intensity activities (22.2% vs 35.1% in males) but higher consumption of fruits and vegetables (p=0.023).
Conclusion: The findings highlight the complex nutritional challenges facing urban adolescents in Dhaka City, characterized by the coexistence of undernutrition and overweight/obesity. Results emphasize the need for comprehensive school-based nutrition programs that address both ends of the malnutrition spectrum while considering gender-specific needs and socioeconomic factors.
Keywords: Adolescent nutrition; Food habits; Nutritional status; School health; Urban health; Bangladesh; BMI-for-age; Dietary diversity; Physical activity
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Student, Public Health, Monroe University Usa and Bachelor of Medicine and Surgery University of Dhaka, , , Bangladesh. Email:  |
Ahmed FA, Sadia SA, Mkpa BO, Afroz S, Islam MT, Food habits and Nutritional status among school-going Adolescents of Dhaka City, Bangladesh. Public Health Rev Int J Public Health Res. 2024;11(2):12-21. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/188 |
 |
 ©
©