Splenic haemangioma - A rare case report
Saritha C.1, Aneela B.2, Mohammed I.3, Chandrasekhar S.4*, S. Sandhya A.5
DOI: https://doi.org/10.17511/ijphr.2016.i1.09
1 Saritha C., Assistant Professor, Kakatiya Medical College, Warangal, Telangana, India.
2 Aneela B., Post Graduate, Kakatiya Medical College, Warangal, Telangana, India.
3 Imranali Mohammed, Assistant Professor, Kakatiya Medical College, Warangal, Telangana, India.
4* Chandrasekhar S., Associate Professor, Kakatiya Medical College, Warangal, Telangana, India.
5 Anil S. Sandhya, Professor, Kakatiya Medical College, Warangal, Telangana, India.
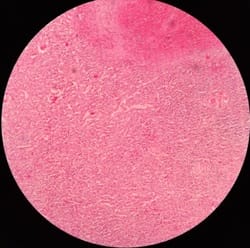
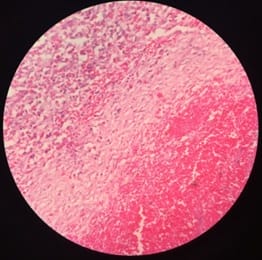
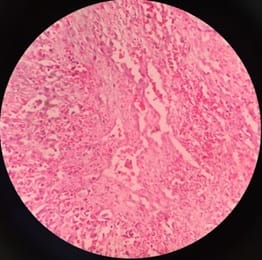
Splenic haemangioma is benign neoplasm of the spleen with fewer than 100 cases reported in the literature. They may represent small, incidental lesions that can produce significant splenomegaly and predispose to splenic rupture. These tumors are rare, usually clinically silent and diagnosed accidentally. We report a case of 65 years old male with haemangioma of spleen presenting as splenomegaly which is extremely rare and deserves a mention.
Keywords: Haemangioma, Spleen, Splenomegaly
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, , Kakatiya Medical College, Warangal, Telangana, India. Email:  |
Saritha C, Aneela B, Mohammed I, Chandrasekhar S, Sandhya AS. Splenic haemangioma - A rare case report. Public Health Rev Int J Public Health Res. 2016;3(1):42-47. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/28 |
 |
 ©
©