Utilization of eye care services among primary school children in urban Kerala
Ann Mary T.1*, Alexander J.2, Patki S.3, Kumar Singh R.4, CH H.5
DOI: https://doi.org/10.17511/ijphr.2016.i2.07
1* Thomas Ann Mary, Assistant Professor, Department of Community Medicine, Sree Narayana Institute of Medical Sciences, Kunnukara, Kerala, India.
2 John Alexander, Professor, Department of Community Medicine, Amrita Institute of Medical Sciences, Kochi, Kerala, India.
3 Swati Patki, Professor, Department of Community Medicine, Sree Narayana Institute of Medical Sciences, Kunnukara, Kerala, India.
4 Rajiv Kumar Singh, Associate Professor, Deparment of Community Medicine, Sree Narayana Institute of Medical Sciences, Kunnukara, Kerala, India.
5 Harsha CH, Assistant Professor, Department of Biostatistics, Sree Narayana Institute of Medical Sciences, Ernakulam, Kerala, India.
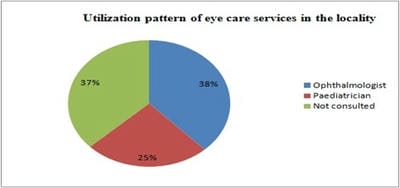
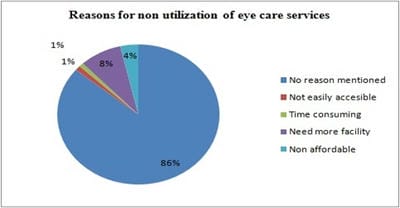
Background: Visual impairment, a major health concern has three main reasons for high prevalence - non-availability, non-accessibility and non-affordability of eye care services. The poor utilization was highlighted as a concern because time interval between eye examinations was high enough for certain avoidable or curable ocular diseases to cause irreversible visual loss. Statistics relating to utilization of eye care services from Kerala and among the primary school children are few in literature. This study was conducted to estimate the pattern of utilization of eye care services for realizing the goal to reduce avoidable blindness by the year 2020. Objective: To assess utilization pattern of eye care services among primary school children. Methods: Cross sectional study in primary school children. Results: Only 35.15% of the students studying in the government and government aided schools had eye care services, their utilization was 94%. Utilization of the eye care service was 63% in the locality. Out of 1100 participants, 222 were not aware of the availability of ophthalmologist. In 523 students with symptoms, 196 (37%) had not consulted a doctor. The predictors for utilizing eye care services in locality were older students, children in private schools. Conclusion: Determining barriers to the use of eye care services is critical for planning strategies to prevent blindness, Health education and counselling can help overcome this problem.
Keywords: Primary school children, Utilization, Visual impairment, Eye care
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Community Medicine, Sree Narayana Institute of Medical Sciences, Kunnukara, Kerala, India. Email:  |
Mary TA, Alexander J, Patki S, Singh RK, Harsha CH. Utilization of eye care services among primary school children in urban Kerala. Public Health Rev Int J Public Health Res. 2016;3(2):82-88. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/36 |
 |
 ©
©