Prevalence and correlates of anemia among elderly population of rural Nalgonda: a cross-sectional analytic study
M Malhotra V.1*, R Kabra P.2, Bhayya S.3, Malhotra R.4
DOI: https://doi.org/10.17511/ijphr.2016.i4.06
1* Varun M Malhotra, Associate Professor, Department of Community Medicine, Kamineni Institute of Medical Sciences, Nalgonda, Telangana, India.
2 Pratyush R Kabra, Assistant Professor, Department of Community Medicine, Kamineni Institute of Medical Sciences, Nalgonda, Telangana, India.
3 Bhayya S, Professor, Department of Community Medicine, Kamineni Institute of Medical Sciences, Nalgonda, Telangana, India.
4 Ritika Malhotra, Aseem Nursing Home, Panchkula, Haryana, India.
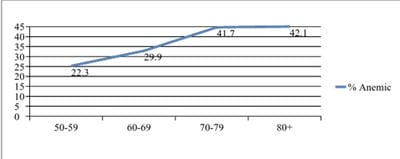
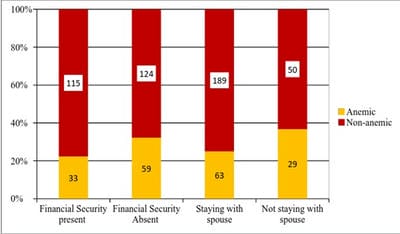
Background: Anemia is a global health challenge, and India is no exception. Large number of studies including NFHS-4 has quantified the prevalence of anemia among children, adolescents, women in reproductive age group, pregnant & lactating mothers and men in age groups below 50 years. However, there is lack of community-based studies among elderly population in India. Objectives: To detect the prevalence of anemia among elderly, and identify socio-demographic and life style factors associated with the disease. Methods: This study was conducted in 11 villages in the jurisdiction of Rural Health Training Centre of a medical college in Nalgonda district of Telangana State. 331 individuals above the age of 50 years of either sex and permanent residents of the villages were included in the study. Haemoglobin levels were detected by Sahli technique. Results: The study revealed that 27.8% (95% CI 23.2-32.8%) of study population was anemic. The prevalence of anemia was significantly higher among females than males. The study showed that prevalence of anemia was associated with advancing age, non-use of footwear, excessive alcohol consumption and history of chronic blood loss. Conclusion: The study indentifies that anemia is a significant public health problem among elderly. The authors recommend that prevalence of anemia among elderly (≥50 years) should be included in future National Family Health Surveys to quantify its prevalence in this demographic group that is progressively increasing in size due to rising longevity.
Keywords: Anemia, Elderly, Nalgonda, Rural
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Community Medicine, Kamineni Institute of Medical Sciences, Nalgonda, Telangana, India. Email:  |
Malhotra VM, Kabra PR, Bhayya S, Malhotra R. Prevalence and correlates of anemia among elderly population of rural Nalgonda: a cross-sectional analytic study. Public Health Rev Int J Public Health Res. 2016;3(4):168-173. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/48 |
 |
 ©
©