A comprehensive study of disease pattern in world’s largest mass gathering
Lal Sahu K.1, Meena S.2, Kumar Singh S.3, Singh Kot L.4*
DOI: https://doi.org/10.17511/ijphr.2017.i2.01
1 Kanti Lal Sahu, Director, Department of Health Syaervices, Government of Madhya Pradesh, Bhopal, Madhya Pradesh, India.
2 Sheela Meena, Integrated Disease Surveillance Program, Department of Health Services, Government of Madhya Pradesh, Bhopal, Madhya Pradesh, India.
3 Shailendra Kumar Singh, Integrated Disease Surveillance Program, Department of Health Services, Government of Madhya Pradesh, Bhopal, Madhya Pradesh, India.
4* Lokendra Singh Kot, State Entomologist and State Epidemiologist respectively, Integrated Disease Surveillance Program, Health Services, Government of Madhya Pradesh, Bhopal, Madhya Pradesh, India.
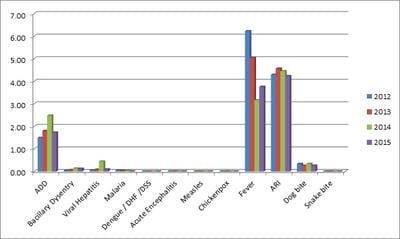
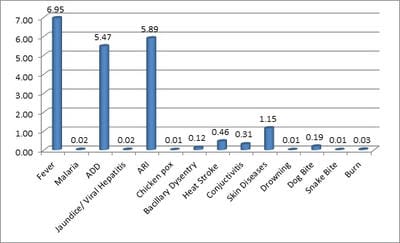
Introduction: A Comprehensive Study of disease pattern in mass gathering of Simhasth Fair in Ujjain city was conducted. Objective of the study were to know the disease trends in a huge event, to know the risk factor triggered by the surveillance system, to assess the importance of health planning and monitoring in a mass gathering and to provide a pathway to future endowers. To provide complete physical, mental and social well being of the pilgrims, state health department established all necessary arrangements. Methods: The period of the data collection of the study was 21 April to 22 May 2016. A stipulated proforma was designed for daily reporting. It was insured that all outbreaks must reported immediately. Analysis and forecasting of the data would be done simultaneously. The data collected on the daily basis. Data were compiled and validated every day. Results: A total of 3,21.841 patients were screened in OPD and 19178 patients were treated as IPD. Highest number of cases recorded of fever i.e. 18,700 (6.95%), followed by acute respiratory infection (ARI), 15,834 (5.89%), Acute diarrheal disease (ADD) 14,715 (5.47%), skin disease 3089 (1.15), heat stroke 1225 (0.46%) and rest shared by injuries 1143 (0.42%), conjunctivitis 823 (0.31%), bacillary dysentery 320 (0.12%), malaria 62 (0.02%), Jaundice/Viral hepatitis 58 (0.02%), chicken pox 21 (0.01%). The cases of dog bite were 504 (0.19%), snake bite 6 (0.01%), Burn 84 (0.03%) and drowning 18 (0.01%). A better planning and forecasting system can provide a solid background to reduce the disease in large gathering.
Keywords: Disease, Surveillance, Mass Gathering, Outbreak, Simhastha Fair
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , State Entomologist and State Epidemiologist respectively, Integrated Disease Surveillance Program, Health Services, Government of Madhya Pradesh, Bhopal, Madhya Pradesh, India. Email:  |
Sahu KL, Meena S, Singh SK, Kot LS. A comprehensive study of disease pattern in world’s largest mass gathering. Public Health Rev Int J Public Health Res. 2017;4(2):31-37. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/59 |
 |
 ©
©