Reproductive and Child Health Programme in Bihar, India: Does Expenditure Matters to Performance?
Kumar A.1*
DOI: https://doi.org/10.17511/ijphr.2014.i2.01
1* Amit Kumar, International Institute for Population Sciences, Mumbai, Maharashtra, India.
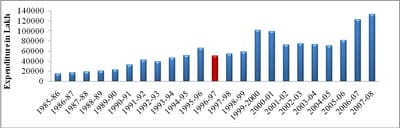
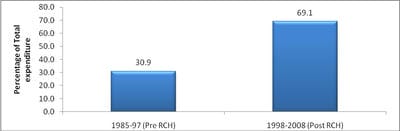
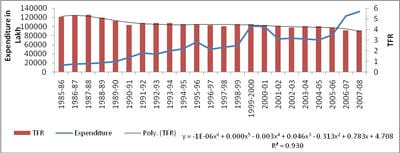
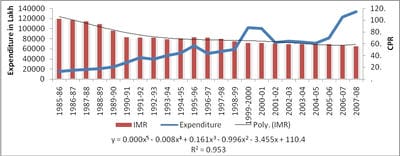
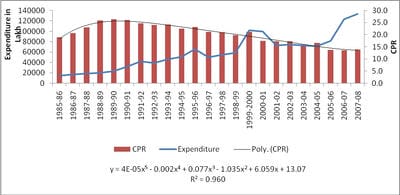
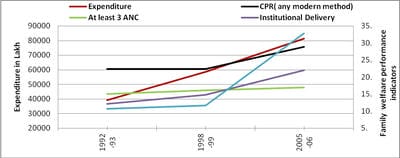
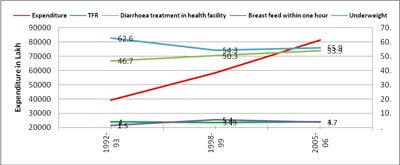
Since the launch of the reproductive and child health policy regime in 1998-99, there has been a massive rise in government expenditure on family welfare programmes in Bihar and national level. This paper makes a systematic effort to assess the performance of the family welfare programmes vis-à-vis trends in expenditure. The trends in key performance indicators for Bihar reveal that progress has been slow and limited in the post-RCH policy regime. Contraceptive prevalence coverage has accelerated, and the increased in the Child immunization and institutional delivery. Consequently, the pace of reduction in the couple protection rate, total fertility rate and infant mortality rate has slowed. It is evidently clear that in the absence of suitable mechanism to operationalise of RCH programme, the exponential increase in expenditure alone cannot lead to commensurate a positive impact on key performance and outcome indicators. There is need suitable mechanism to operationalise RCH programme.
Keywords: Child health, Expenditure, Family Planning, Performance, Reproductive Health
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , International Institute for Population Sciences, Mumbai, Maharashtra, India. |
Kumar A. Reproductive and Child Health Programme in Bihar, India: Does Expenditure Matters to Performance?. Public Health Rev Int J Public Health Res. 2014;1(2):45-60. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/7 |
 |
 ©
©