An analysis of health seeking behaviour on utilization of skilled delivery services by Maasai women in kiekonyokie sub location of kajiado county in Kenya
Lebahati Simel L.1, Nanduri L.2, A. Juma P.3, O. Omuga B.4*
DOI: https://doi.org/10.17511/ijphr.2017.i5.06
1 Laban Lebahati Simel, Lecturer, School of Public Health, Asmara College of health Science, Asmara, Eritrea, East Africa.
4* Lakshmi Nanduri, Associate Professor, School of Public Health, Asmara College of health Science, Asmara, Eritrea, East Africa.
2 Pamela A. Juma, Director Great Lakes University of Kisumu, Nairobi Campus, Nairobi, Kenya.
3 Blasio O. Omuga, Lecturer, University of Nairobi, Nairobi, Kenya.
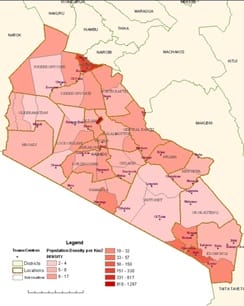
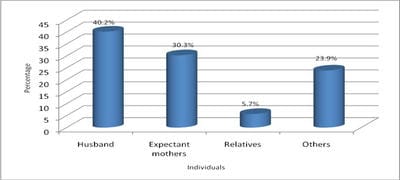
Introduction: Maternal health is one of the eight Millennium Development Goals, is central to poverty reduction and overall development, and it increased international attention for monitoring progress on maternal health and improving access to skilled attendants at deliveries. In Kenya, 44 percent of births are delivered under the supervision of a health professional, mainly a nurse or midwife. Objectives: This research paper aimed to analyse the role of Health Seeking Behaviour on the utilization of skilled delivery services by Maasai women, the study population belonging to a community of nomadic life style in North of Kajiado County in Kenya. Methodology: The study design was a cross sectional descriptive study adopting both quantitative and qualitative methodologies. The sample size was 264 women of reproductive age obtained by using formula given by Fisher et al., when the population is more than 10,000. The quantitative data has been analyzed using (SPSS) version 17.0 while the qualitative data was analyzed by summarizing of the themes. Results: Results show that 57.2% Maasai women go to the health facility in case of illnesses, while 7.6% consulted their mother in law., husbands make most of the decisions (40.2%) on the place of delivery of the expectant mothers whereas as the relatives make the least decisions 5.7%. Preparation of the expectant mother for delivery did not have a statistical significant p-0.046.The traditional rite of passage practices had no statistical significance p-0.190. 72% of womencould mention at least one correct danger sign for pregnancy out of the posssible four.
Keywords: Maasai Women, Health Seeking Behaviour, Utilization of Skilled Delivery Services, Kajiado County, Kenya
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, School of Public Health, Asmara College of health Science, Asmara, Eritrea, East Africa. Email:  |
Simel LL, Nanduri L, Juma PA, Omuga BO. An analysis of health seeking behaviour on utilization of skilled delivery services by Maasai women in kiekonyokie sub location of kajiado county in Kenya. Public Health Rev Int J Public Health Res. 2017;4(5):134-140. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/74 |
 |
 ©
©