Study of cross-referrals between Integrated Counselling & Testing Centre and RNTCP-Designated Microscopy Centre at a tertiary care hospital in Bengaluru, Karnataka
V S.1, S.S. Vidusha K.2, A.C. S.3*
DOI: https://doi.org/10.17511/ijphr.2019.i1.02
1 Srividya V, Associate Professor, Department of Community Medicine, Rajarajeswari Medical College and Hospital, Bangalore, Karnataka, India.
2 Karavadi S.S. Vidusha, Assistant Professor, Department of Community Medicine, Rajarajeswari Medical College and Hospital, Bangalore, Karnataka, India.
3* Shyam A.C., Professor, Department of Community Medicine, Rajarajeswari Medical College and Hospital, Bangalore, Karnataka, India.
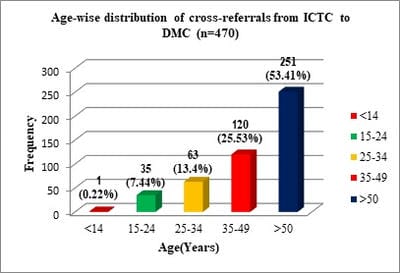
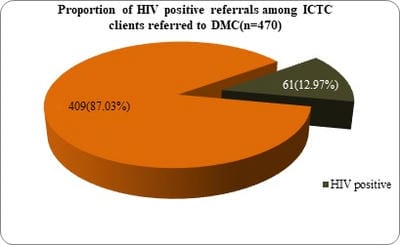
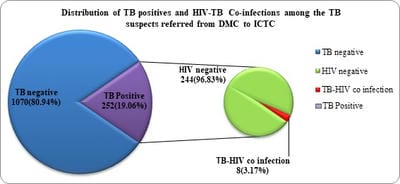
Introduction: HIV and TB infections continue to fuel and amplify each other. The present study was designed to assess the socio-demographic profile of the clients visiting ICTC and to assess the pattern of cross referrals between ICTC and RNTCP Designated Microscopy Centre at a private medical college in Bengaluru, Karnataka. Materials & Methods: This was a descriptive study comprising of all the clients visiting ICTC and TB Suspects visiting RNTCP DMC during the study period from April to December 2018. Data entry was done in MS excel and analyzed in SPSS software. Results: A total of 9405 clients visited ICTC during the study period, 68(0.73%) of them were diagnosed to be HIV positive. HIV Seropositivity was found to be higher among 35-49 yrs age group 28(41.17%), male clients 37(54.41%) and among semiskilled workers 19(27.94%) followed by housewives 18 (26.50%). There were 9 HIV concordant couples. 252(19.06%) of the TB suspects visiting the DMC were TB positive. 8(3.17%) clients had HIV-TB Co-infection. Statistically significant association was observed between HIV status and TB status of the study subjects (p <0.05). Conclusion: ICTC is an excellent site for both HIV testing and screening for TB. Similarly, RNTCP DMC is instrumental in TB case finding and also for detecting individuals at high risk for HIV seropositivity. Appropriate cross referral between these two centres plays a pivotal role in reducing the burden of both infections.
Keywords: Cross referrals, Designated Microscopy Centre, HIV, RNTCP, TB
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Community Medicine, Rajarajeswari Medical College and Hospital, Bangalore, Karnataka, India. Email:  |
Srividya V, Vidusha KSS, Shyam AC. Study of cross-referrals between Integrated Counselling and Testing Centre and RNTCP-Designated Microscopy Centre at a tertiary care hospital in Bengaluru, Karnataka. Public Health Rev Int J Public Health Res. 2019;6(1):9-16. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/95 |
 |
 ©
©