A cross-sectional study correlating serum calcium levels and the state of control of Type 2 Diabetes Mellitus
Ganesan H.1, Arumugham Dhanaraj S.2*, Aishwarya T.3
DOI: https://doi.org/10.17511/ijphr.2019.i6.06
1 Harissh Ganesan, M.B.B.S. Student, Government Villupuram Medical College and Hospital, Tamilnadu, India.
2* Saravanakumari Arumugham Dhanaraj, Assistant Professor, Department of Community Medicine, Government Villupuram Medical College and Hospital, Tamilnadu, India.
3 T N Aishwarya, M.B.B.S. Student, Government Villupuram Medical College and Hospital, Tamilnadu, India.
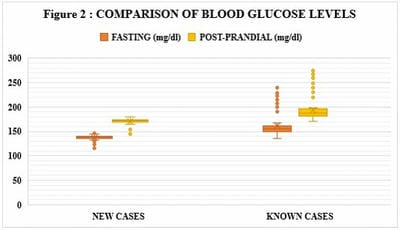
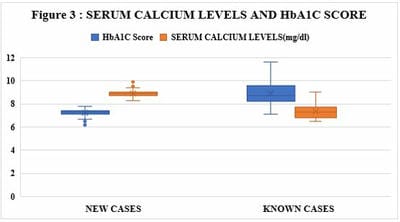
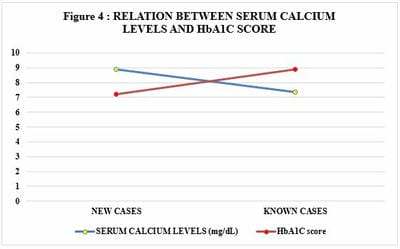
Calcium plays a major role in secreting insulin in our body other than its various other function, the correlation of calcium and Type 2 Diabetes mellitus is a concept that needed much more justification and evident scientific proofs. This research aimed to study the association of serum calcium levels with Type 2 Diabetes Mellitus. Methodology: A total of 351 patients were included in this study which included both newly diagnosed cases of Type 2 Diabetes Mellitus and already known cases of Type 2 Diabetes Mellitus. The study parameters- Fasting blood glucose, post-prandial blood glucose, HbA1C score and Serum Calcium Levels were analysed. Results: The Fasting blood glucose levels and post-prandial blood glucose levels of known cases of Type 2 Diabetes Mellitus were 160.89 ± 22.60 mg/dL and 194.33 ± 22.70 mg/dL and that of newly diagnosed cases were 137.90 ± 4.21 mg/dL and 171.48 ± 4.59 mg/dL respectively. The HbA1C score in newly diagnosed cases was 7.20 ± 0.30 and that of known case was 8.90 ± 1.04. The Serum Calcium levels of the newly diagnosed cases was 8.87 ± 0.26 mg/dL and 7.36 ± 0.64 mg/dL for the already known cases. Conclusion: Changes in serum calcium levels are associated with the risk of T2DM in an Indian population. Thereby the patients with T2DM have to be supplemented with calcium which would help in progression of the disease furthermore.
Keywords: Type 2 Diabetes Mellitus, Serum Calcium Levels, Incidence of Diabetes, Level of control of Diabetes
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Community Medicine, Government Villupuram Medical College and Hospital, , Tamilnadu, India. Email:  |
Harissh Ganesan, Saravanakumari Arumugham Dhanaraj, T N Aishwarya, A cross-sectional study correlating serum calcium levels and the state of control of Type 2 Diabetes Mellitus. Public Health Rev Int J Public Health Res. 2019;6(6):246-251. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/183 |
 |
 ©
©