The Impact of Air Pollution Controls on Health and Health Inequity Among Middle-Aged and Older-A Cross-Sectional Study
Mkpa BO1*, Ahmed FA2
DOI:https://doi.org/10.17511/ijphr.2025.i01.01
1* Beatrice Onyinyechi Mkpa, Student, Public Health, Monro University, USA.
2 Ferdous Ara Ahmed, Student, Medicine and Surgery, University of Dhaka, Dhaka, Bangladesh.
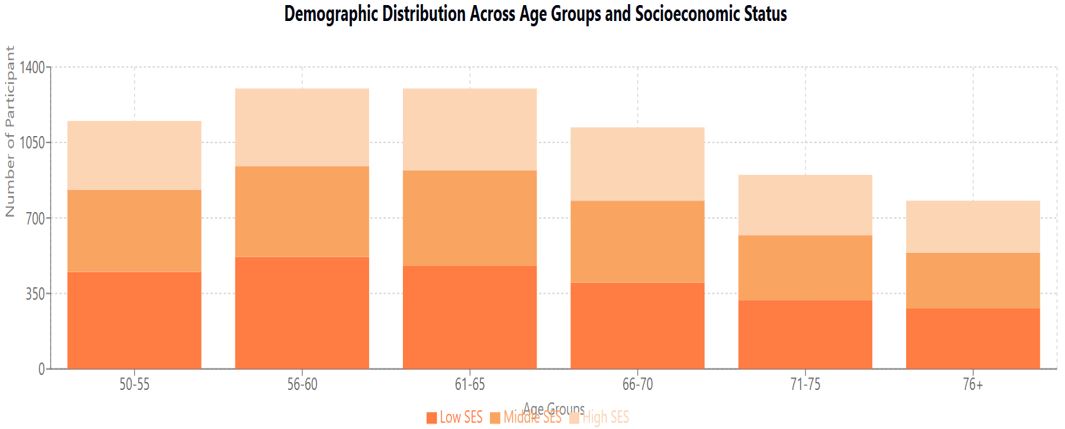
Background: Air pollution remains a significant public health concern, particularly affecting middle-aged and older populations. This study investigates the impact of air pollution control measures on health outcomes and health inequities among 5,000 individuals aged 50 and above.
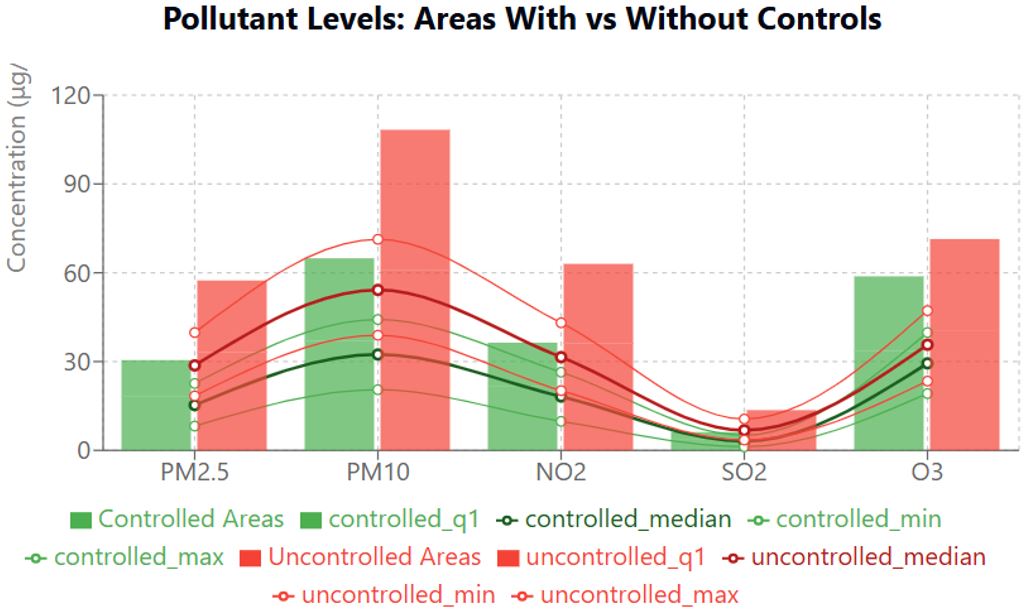
Methods: A cross-sectional study was conducted between 2020 and 2023, analyzing data from urban and suburban areas with and without implemented air pollution controls. Air quality was monitored using EPA stations and portable monitors, measuring PM2.5, PM10, NO2, SO2, and O3. Health outcomes were assessed through medical records, standardized questionnaires, clinical examinations, and lung function tests. Socioeconomic status was evaluated using validated instruments, and the effectiveness of control measures was assessed using the Environmental Policy Implementation Index.
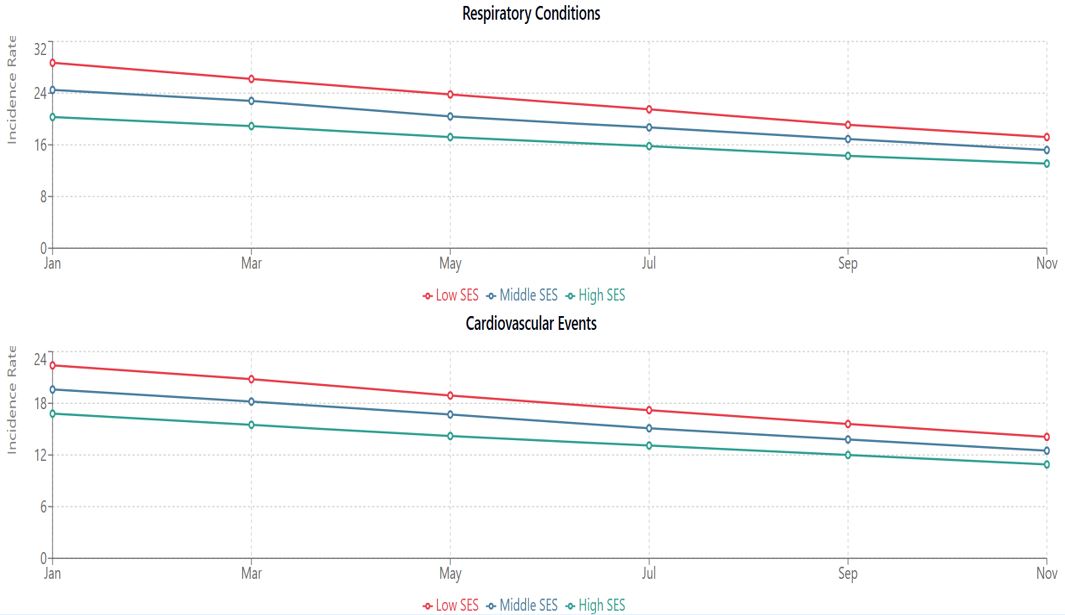
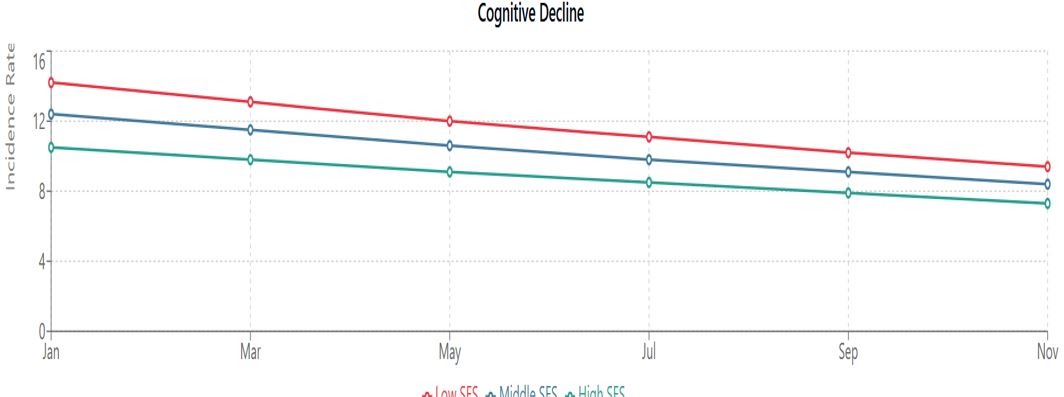
Results: Implementation of air pollution controls was associated with significant health improvements across all socioeconomic groups. Areas with controls showed lower mean annual PM2.5 concentrations (15.3 ± 4.2 μg/m³ vs 28.7 ± 6.8 μg/m³, p<0.001) and reduced incidence of respiratory conditions (15.2% vs 28.7% in lower SES groups; 12.1% vs 20.3% in higher SES groups). The Concentration Index improved from 0.48 to 0.32 (p<0.001), indicating reduced health inequities. Industrial controls demonstrated the highest effectiveness (25.9% improvement), followed by emission controls (23.5%) and traffic management measures (18.7%).
Conclusions: Air pollution control measures effectively improve health outcomes among middle-aged and older adults, with varying benefits across socioeconomic groups. While overall health inequities decreased, persistent disparities suggest the need for targeted interventions in disadvantaged communities. These findings support strengthening air quality regulations while emphasizing equity-focused implementation strategies.
Keywords: Air pollution; Environmental policy; Health equity; Aging population; Public health; Environmental justice
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Student, Public Health, Monro University, , , USA. Email:  |
Mkpa BO, Ahmed FA, The Impact of Air Pollution Controls on Health and Health Inequity Among Middle-Aged and Older-A Cross-Sectional Study. Public Health Rev Int J Public Health Res. 2025;12(1):1-8. Available From https://publichealth.medresearch.in/index.php/ijphr/article/view/193 |
 |
 ©
©